We know the name, and we know we need to watch our cholesterol levels, but what is cholesterol?
Cholesterol is a waxy substance that is made by your liver and also comes from foods we eat. Your body needs small amounts of cholesterol to build cells and make vitamins and other hormones. But most of us have too much cholesterol that can wreak havoc in our arteries, including coronary, carotid, and peripheral arteries leading to the development of plaque and blockages, putting us at risk for heart attack, stroke, or even sudden death.
Cholesterol comes from two sources. Your liver makes all the cholesterol you need and oftentimes more than you require. The production of cholesterol by the liver is in large part under genetic control and inherited from our parents. The remainder of the cholesterol in your body comes from animal sources. For example, meat, poultry, and dairy products all contain dietary cholesterol. Those same foods are high in saturated and trans fats. These fats cause your liver to make more cholesterol than it otherwise would. For some people, this added production means they go from a normal cholesterol level to one that’s unhealthy. Some tropical oils such as palm oil, palm kernel oil, and coconut oil – contain saturated fat that can increase bad cholesterol. These oils are often found in baked goods.
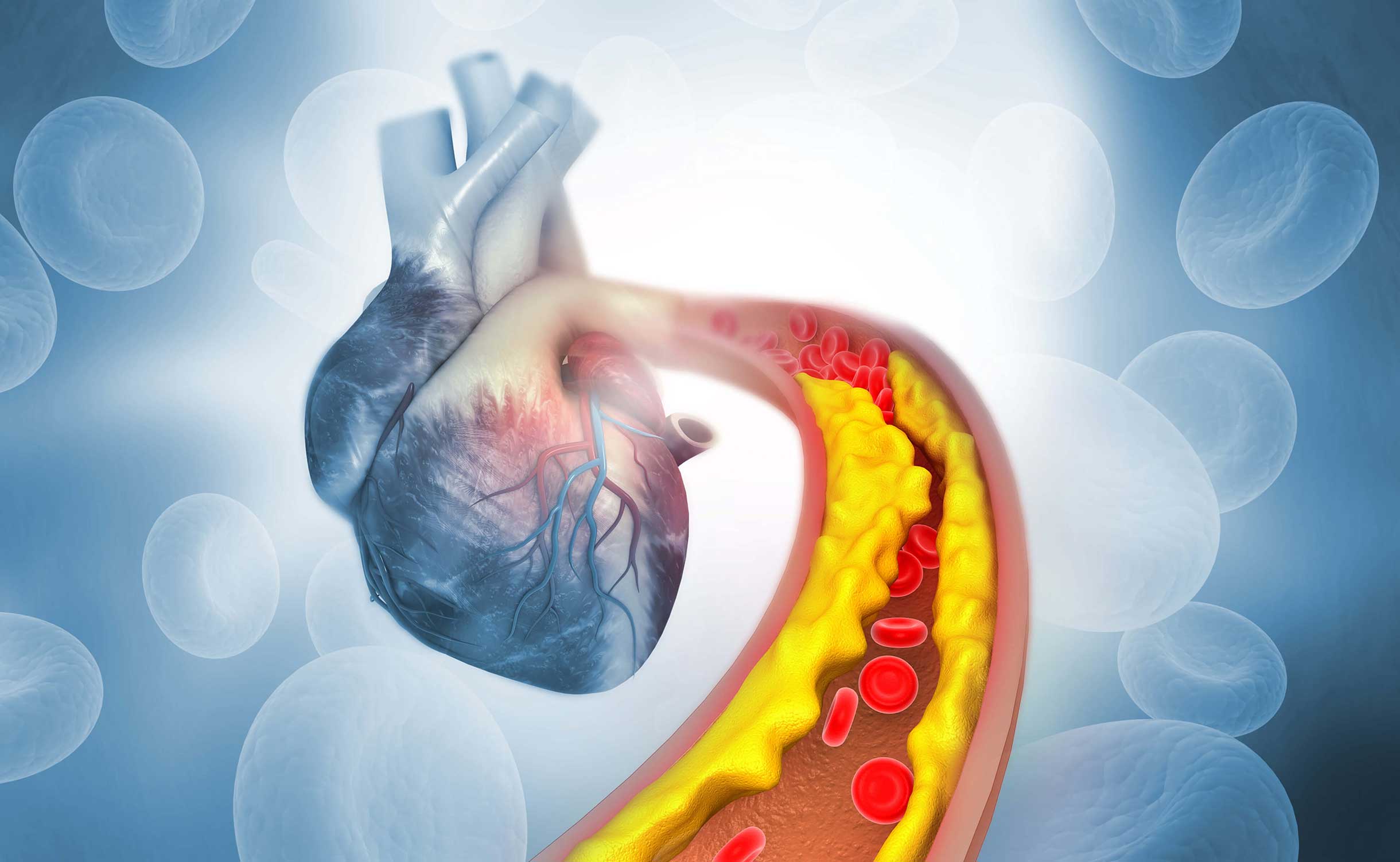
85% of the cholesterol in our body is made by the liver, which is why diet and exercise, though important, may not be enough to lower our cholesterol to desired levels. Cholesterol circulates in the blood, and as it bathes the inner surface of the arteries, it is absorbed into the wall of the artery leading to a process similar to “rusting” called atherosclerosis. As the amount of cholesterol in your blood increases, so does the risk to your cardiovascular health. That’s why it’s important to have your cholesterol tested, so you can know your levels and that you ask your healthcare professional what an ideal cholesterol for you would be based on your personalized risk of heart attack and stroke. The higher your risk, the lower your cholesterol level should be.
There are multiple types of cholesterol, including LDL cholesterol, which is bad, and HDL, which is sometimes good and sometimes not, triglyceride, which is the fatty cholesterol, and lipoprotein a, which is the horrible cholesterol. LDL cholesterol is considered the “bad” cholesterol because it contributes to fatty buildup in arteries. HDL cholesterol can be thought of as the “good” cholesterol because a healthy level may protect against heart attack and stroke. HDL carries LDL (bad) cholesterol away from the arteries and back to the liver, where the LDL is broken down and passed from the body. Triglycerides are the most common type of fat in the body. They store excess energy from your diet. A high triglyceride level combined with high LDL (bad) cholesterol or low HDL (good) cholesterol is linked with fatty buildups within the artery walls, Lipoprotein a is a cholesterol that many have not heard much about, but it is a horrible cholesterol as it increases the risk heart attack, stroke and a heart valve condition called aortic stenosis. Lipoprotein a, also referred to as LPa, is inherited in an autosomal dominant fashion, so it is important to be sure that relatives of people with high levels of LPa should have a simple blood test to determine if they are at risk.
People who have suffered from more advanced cardiovascular disease and have had a heart attack, stroke, peripheral artery disease or bypass surgery, or stent procedure need to have their bad cholesterol, LDL, down to below 55 mg/dl in many cases. Patients with diabetes or who have evidence of plaque formation seen on screening tests such as a coronary calcium score, coronary CT angiogram, or carotid ultrasound need their LDL levels to be below 70 mg/dl. Basically, when it comes to LDL cholesterol levels, lower is better. For every 2% one lowers their LDL level, they lower their chance of heart attack and stroke by 1% so a 50% reduction of LDL leads to a 25% reduction of risk. Often times patients and even their healthcare professionals are concerned that cholesterol levels could be too low. This is most often not the case as infants have LDL levels of 30 mg/dl. We know from clinical trial studies that we can actually get regression of cholesterol deposits if we achieve LDL levels < 50 mg/dl.
Though lifestyle modifications, such as regular exercise, including aerobic and weight bearing, should be deployed in patients who have either suffered from the complications of atherosclerosis or are at high risk, in the vast majority of cases, they will not be able to achieve recommended cholesterol levels. That is when medical therapy is called on to get us “to the promised land” of cholesterol goals. Statins are a family of medications that are most commonly used to lower cholesterol levels. Most statins are generic, so they are inexpensive and can safely lower LDL by as much as 50%. The most common side effect is muscle (not joint) achiness that resolves with a dose reduction, changing to another statin, or by stopping the drug. Other medical treatments include ezetimibe, which reduces the absorption of cholesterol from our intestines, bempedoic acid, or Nexletol, a newer medication that has been shown to be very useful in statin intolerance patients and the family of “injectable” medications that block a protein called PCSK9 that gets in the way of our bodies ability to break down cholesterol. These medications can be given as an easy-to-administer subcutaneous injection twice a week (Repatha, Praluent) or twice a year (Leqvio). Vascepa is a unique medication that lowers triglyceride levels as an Omega-3 EPA oil and also has been found to lower the risk of heart attack and stroke. Over-the-counter fish oils are not recommended for heart disease prevention due to the presence of impurities. There are no commercially available treatments targeted to lipoprotein (a).
Even with the treatments mentioned above, most patients are not able to get to recommended cholesterol goals and remain at heightened risk of heart attack, stroke, and sudden death. In some patients, the medications are not strong enough, not tolerated or not covered by insurance, and are too expensive. We are fortunate at the National Heart Institute (NHI) to have as one of our goals to find newer, more effective, and safer treatments through our clinical trial programs. We are continually evaluating new treatments that lower LDL-cholesterol, triglycerides, and lipoprotein a levels. Also, knowing how much inflammation plays a role in atherosclerosis and evaluating novel treatments that reduce the concentrations of inflammatory proteins such as interleukin 6 is a key area of focus.
If you have been diagnosed with a cholesterol disorder or have issues related to plaque in your arteries, feel free to reach out to the National Heart Institute, a center of excellence for clinical trials, to answer any questions and provide information on our currently enrolling clinical trials.
Our expert physician investigators and bilingual research staff will work with you and your healthcare team to select the best trial for you. There is no cost for participating in a clinical trial; if selected, most trials provide payments for each study site visit and assistance with transportation.
To learn learn more, contact us at: info@nationalheartinstutute.org.
We’re here to help and make a difference!
Cholesterol Disorders: The Good, The Bad & The Terrible!
By Norman E. Lepor, MD, FACC FAHA
|July 27, 2023
|Share